Get Premium
Dark mode theme is available exclusively for premium users. Learn more about the benefits of subscribing.
No fees, cancel anytime.

 Dark Mode Ad-Free Browsing Unlimited Content
Dark Mode Ad-Free Browsing Unlimited Content 
 Ad-Free Browsing Unlimited Content Dark Mode
Ad-Free Browsing Unlimited Content Dark Mode 
Join 1.2 million Panda readers who get the best art, memes, and fun stories every week!
If your workplace's walls could talk, what would they say? I guess it largely depends on your profession. The morgue, for example, might reveal very different secrets to the hair salon or the tech support call center...
One place that holds a rollercoaster of stories is a hospital. Life-changing moments happen here every single day. But what patients and their families see or hear pales in comparison the reality experienced by the staff who work in these buildings. Doctors, nurses, paramedics, and even janitors are privy to things that might surprise even the most hardcore Grey's Anatomy fan.
They've been spilling some secrets online, in response to someone asking, "What are the unspoken (dark) realities of medicine that surprised you most?" From battles with mental health and substance use to admissions that medical professionals are merely making "educated guesses," each answer takes us deeper into the minds of those who have chosen to save lives for a living. Bored Panda has put together a list of the best ones below. Don't forget to upvote your favorites.
This post may include affiliate links.
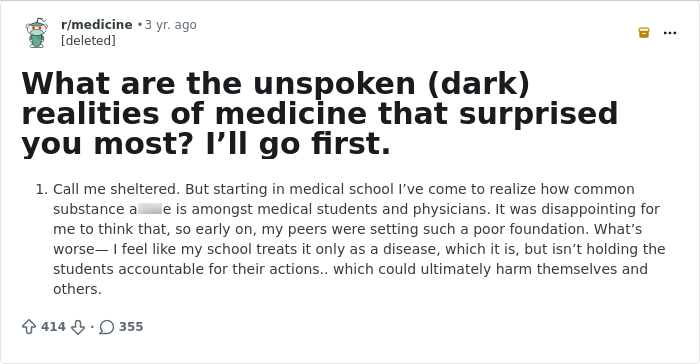
 I honestly expected everyone to be the pinnacle of maturity and professionalism.
I honestly expected everyone to be the pinnacle of maturity and professionalism.
Boy was I wrong.
We turn to our trusted medical professionals to help us in times of need, but many of them are facing crises of their own.
According to the Centers for Disease Control, health workers are feeling fatigue, loss, and grief at levels higher than before the Covid pandemic. And reports of poor mental health symptoms have increased more for health workers than for other worker groups.
The Pew Research Center reveals that physicians, nurses, health technicians, and others in the sector are at increased risk of taking their own lives, compared with their nonmedical peers.
One U.S. study found that 14% of healthcare workers had reported having such thoughts, 6% had gone as far as planning the act, and 3.5% had followed through by attempting it. Sadly, every year, more than 300 physicians are successful in taking their own lives.
 The dissociation between patient's clinical state and some conditions.
The dissociation between patient's clinical state and some conditions.
For example, septic patients. Sometimes they're fully conscious in the morning, they crash and get ventilated in the evening and they die in the middle of the night.
Not only this is disheartening, this can lead to conflicts with their relatives - "But doc, he was just fine yesterday! We talked on the phone! This is probably malpractice!".
Even with the stakes this high, experts say healthcare nurses are less likely to seek mental health support when experiencing depressive thoughts compared with nurses who do not have such thoughts.
"And in contrast to the general population, physicians are less likely to seek mental health support even when experiencing [thoughts of self-harm]," adds the Pew site.
One of the reasons for this is the stigma attached to mental health issues within the medical fraternity. Some fear their careers will suffer if they speak up. A 2021 study found that 47% of doctors agreed that doctors with a history of depression or anxiety disorder are less likely to be hired or appointed.
 How often mistakes are made, even with the whole swiss cheese model and adoption of checklists and EHR. What's surprised me even more was how few were getting caught or recognized, even after the fact.
How often mistakes are made, even with the whole swiss cheese model and adoption of checklists and EHR. What's surprised me even more was how few were getting caught or recognized, even after the fact.
It would help to have a no blame culture, but given how malpractice works, that's not going to happen anytime soon. I thought for awhile that residents might start getting more sleep, but COVID destroyed any hope of that.
 If you sit there on your phone the whole time the mother of your child is in labor such that a nurse has to step in and fulfill the supportive role instead, yeah everyone knows and you’re getting judged by the whole unit.
If you sit there on your phone the whole time the mother of your child is in labor such that a nurse has to step in and fulfill the supportive role instead, yeah everyone knows and you’re getting judged by the whole unit.
Pew adds that in many U.S. states, health care providers applying for their license or credentials must disclose whether they have ever had mental health concerns or received mental health care.
"Data shows that 40% of physicians and 35% of physicians assistants reported reluctance to seeking mental health supports because of concerns about licensure repercussions," reveals the site, adding that many nurses also worry about the professional consequences of receiving mental health care.
 Clinical practice isn’t really evidence based, a lot of things we do mostly because it’s the way it’s always been done. There is so much we don’t know about medicine and most of the time we are taking educated guesses. Most diagnosis and treatment plans are a risk/ benefit analysis of probabilities with a significant (more than 5%) error rate. We are just not that good at medicine yet.
Clinical practice isn’t really evidence based, a lot of things we do mostly because it’s the way it’s always been done. There is so much we don’t know about medicine and most of the time we are taking educated guesses. Most diagnosis and treatment plans are a risk/ benefit analysis of probabilities with a significant (more than 5%) error rate. We are just not that good at medicine yet.
There is a large discrepancy in the publics expectation of how accurate we are and the reality. I think in 100 years we will look back at the barbaric way we practice medicine currently even in our best institutions. To give an example the best treatment we have figured out for resistant depression is shocking our patients, it works well and it’s the best we have.
 As another perspective to what you've witnessed, substance use treatment is remarkably effective for physicians. Having a multimillion dollar career on the line is an enormous incentive to get treated. The only other demographic with as high a rate of treatment success for substance use is pilots, likely for similar reasons. Something like 90% of physicians who seek treatment for substance use are abstinent 10 years later.
As another perspective to what you've witnessed, substance use treatment is remarkably effective for physicians. Having a multimillion dollar career on the line is an enormous incentive to get treated. The only other demographic with as high a rate of treatment success for substance use is pilots, likely for similar reasons. Something like 90% of physicians who seek treatment for substance use are abstinent 10 years later.
 How little we can do for seriously mentally ill, demented, or chronically encephalopathic patients. They run into a vicious cycle of getting hospitalized and then unable to be discharged because they can't take care of themselves and no place will accept them because of their behavior and they are mentally incompetent and can't be released by choice. They don't get better. There's a point of no return in mental illness.
How little we can do for seriously mentally ill, demented, or chronically encephalopathic patients. They run into a vicious cycle of getting hospitalized and then unable to be discharged because they can't take care of themselves and no place will accept them because of their behavior and they are mentally incompetent and can't be released by choice. They don't get better. There's a point of no return in mental illness.
48% of doctors who took part in a 2023 poll reported that they know a physician, colleague, or peer who said they would not seek mental health care. This is despite more than half reporting that they know of a physician who has considered, attempted, or died by taking their own life.
A separate survey found that only 26% of physicians with mental health conditions seek treatment.
 How many policy decisions that seem like they are well-intentioned are to covertly affect behavior in often malintentioned ways. Making portal messaging intentionally difficult to stop patients from creating more work. Setting scheduling up purposely to make it harder for patients with minimally severe complaints to schedule. Peer enforcement policies that make physicians police each other or make an individual feel guilty or inferior, so they will work harder or not speak out against things that cross work-life boundaries, capitalizing on physicians’ insecurities and taking advantage of their charitable attitude.
How many policy decisions that seem like they are well-intentioned are to covertly affect behavior in often malintentioned ways. Making portal messaging intentionally difficult to stop patients from creating more work. Setting scheduling up purposely to make it harder for patients with minimally severe complaints to schedule. Peer enforcement policies that make physicians police each other or make an individual feel guilty or inferior, so they will work harder or not speak out against things that cross work-life boundaries, capitalizing on physicians’ insecurities and taking advantage of their charitable attitude.
Second one would be the above, but during conversations centered on financial gain/cost reduction.
 How a single fall, and subsequent hip fracture for an elderly individual can be a death sentence for so many.
How a single fall, and subsequent hip fracture for an elderly individual can be a death sentence for so many.
 At some stage most consultant physicians stop learning, adapting or developing their clinical practice. They also mostly practice based on heuristics (especially availability and familiarity heuristics). This form of practice is likely to handle most things in a decent enough way that is acceptable at a certain time and place. However it restricts the physician from thinking laterally, dealing with new or complex situations, or becoming truly exceptional.
At some stage most consultant physicians stop learning, adapting or developing their clinical practice. They also mostly practice based on heuristics (especially availability and familiarity heuristics). This form of practice is likely to handle most things in a decent enough way that is acceptable at a certain time and place. However it restricts the physician from thinking laterally, dealing with new or complex situations, or becoming truly exceptional.
There are a handful of exceptions to this and continue to develop their skills and knowledge. These clinicians have all had a habit of regularly reading journal articles, listening to podcasts or being involved in academia themselves. It’s hard to know if it’s the latest research that is having a positive effect on their practice OR if the kind of clinicians who are regularly working on themselves happen to have a habit for reading articles.
“Health workers are experiencing unprecedented rates of burnout and mental health conditions due to factors like long, irregular hours, unsafe and difficult work environments, resource shortages, and high clinical demands they face daily,” says Stefanie Simmons, chief medical officer of the Dr. Lorna Breen Heroes’ Foundation.
But the mental health crisis within the medical profession is not only impacting doctors, nurses and their peers. It can also affect the treatment that patients receive, or don't receive.
“Many of the operational policies and practices are there based on the misplaced belief that they protect patient safety, but the reality is starkly different: When health workers fear seeking help, the quality of care declines, mental health conditions and burnout intensify, workforce shortages grow, and lives are lost,” warns Simmons.
 4-5% of doctors who leave the field of medicine each year do so by ending their lives. We as a profession suck at mental health among ourselves.
4-5% of doctors who leave the field of medicine each year do so by ending their lives. We as a profession suck at mental health among ourselves.
 Hospitals are very hesitant to discipline surgeons who have bad skills even though they are a danger to patients because surgery is where hospitals make their profits.
Hospitals are very hesitant to discipline surgeons who have bad skills even though they are a danger to patients because surgery is where hospitals make their profits.
 Maybe someone can answer this, but how closed minded some physicians are to alternative careers, or interests that aren’t clinical medicine.
Maybe someone can answer this, but how closed minded some physicians are to alternative careers, or interests that aren’t clinical medicine.
I couldn’t speak about my passions and interest in not practicing medicine during med school. I had people get wiffs and it was scary. Like another poster said, I assumed way more maturity in this field.
 “Discharge to street” dispos. Really really unsettling feeling to take a bed and four walls away from someone so we can treat someone else.
“Discharge to street” dispos. Really really unsettling feeling to take a bed and four walls away from someone so we can treat someone else.
 Just how many nurses just go through the motions of scientific thought and continue to believe in lies, like astrology, or that vaccines don't work or that vaccines cause harm, or that evolution isn't real.
Just how many nurses just go through the motions of scientific thought and continue to believe in lies, like astrology, or that vaccines don't work or that vaccines cause harm, or that evolution isn't real.
That the people who take care of our elderly are extremely underpaid and overworked.
How many patients just don't GAF what happens to them.
 In a small town hospital I used to work in, there was a gyno who would show up to work visibly drunk. Everyone knew, no one did anything until the guy came to work the ER so wasted he had to be hidden from the patients, rehydrate and sent home to avoid a scandal
In a small town hospital I used to work in, there was a gyno who would show up to work visibly drunk. Everyone knew, no one did anything until the guy came to work the ER so wasted he had to be hidden from the patients, rehydrate and sent home to avoid a scandal
Another physician had a decent amount of malpractice suits, he was legally ordered to stop practicing medicine there while investigation were underway. The dude didn't give a s**t, he just showed up to work for months and everyone around him did nothing because he was the chief of surgery. He only complied when someone denounced to the judges he was still there
I'm sure s**t like this goes on in a lot of hospitals, and due to this archaic code of honor among peers thing a lot of people do not dare to say anything for fear of retaliation.
 How old so many young people are from lifestyle and uncontrolled diseases. People in their mid 40s who look 80 with multiple amputations, bed sores, multiple cardiac stents from uncontrolled diabetes and obesity, etc. Being raised in a middle class setting where people weren't perfect but generally were active, went to the PCP, maybe carried some extra weight but generally took care of themselves, the degree to which this happens in other populations is shocking. The people I know from my personal life in their 70s are way healthier than the average middle aged patient in the inner city clinic where I trained and it's not even close.
How old so many young people are from lifestyle and uncontrolled diseases. People in their mid 40s who look 80 with multiple amputations, bed sores, multiple cardiac stents from uncontrolled diabetes and obesity, etc. Being raised in a middle class setting where people weren't perfect but generally were active, went to the PCP, maybe carried some extra weight but generally took care of themselves, the degree to which this happens in other populations is shocking. The people I know from my personal life in their 70s are way healthier than the average middle aged patient in the inner city clinic where I trained and it's not even close.
 How many physicians practice counter to well-evidenced guidelines. I'm not obsessed with guidelines, mind you-- they can get out of date quickly. I'm talking about sturdy ones. It astonishes me how rampant it is for practices to do strep swabs on kids with obvious URI symptoms, even before the patients are seen. I'm not talking about kids who seem to possibly have more than one thing going on-- I know Hickam's Dictum. I'm talking about kids with colds and nothing suspicious for strep.
How many physicians practice counter to well-evidenced guidelines. I'm not obsessed with guidelines, mind you-- they can get out of date quickly. I'm talking about sturdy ones. It astonishes me how rampant it is for practices to do strep swabs on kids with obvious URI symptoms, even before the patients are seen. I'm not talking about kids who seem to possibly have more than one thing going on-- I know Hickam's Dictum. I'm talking about kids with colds and nothing suspicious for strep.
I taught students for years, and I know they know this is wrong and why when they leave. I know they learn pretest probability. I know they understand the harms of inappropriate antibiotics. It's not rocket science. But it seems like they mostly go out and ignore the existence of the common cold.
I have done private practice more years than I taught, and no, it's not hard or time consuming to explain this stuff to patients. I do it every working day. Once I've explained the first time, I don't have to repeat it. I've had rare parents get upset and leave but if we all followed the science, even that wouldn't happen. Parents appreciate honesty, and I have "grand-patients", children of former patients.
Peer pressure is not a good excuse. We have an ethical responsibility towards our patients.
I do not think I will ever understand how seemingly intelligent and well educated people can do this nonsense. It makes me lean towards absurdism sometimes, as a life philosophy.
 Sometimes when people die we just put an oxygen mask on them and wheel them through the corridors. Less distressing for other patients and visitors to think they are asleep rather than see a body with a sheet over it.
Sometimes when people die we just put an oxygen mask on them and wheel them through the corridors. Less distressing for other patients and visitors to think they are asleep rather than see a body with a sheet over it.
 You are doing your 90 year old grandmother a great disservice by making her a full code, she will not survive CPR and her death will be significantly more traumatic because of it.
You are doing your 90 year old grandmother a great disservice by making her a full code, she will not survive CPR and her death will be significantly more traumatic because of it.
 Some families reject death so much, they beg the doctors and nursing staff to do lifesaving measures on their 95 year old grandma who has cancer everywhere and is begging for death. It's just unacceptable.
Some families reject death so much, they beg the doctors and nursing staff to do lifesaving measures on their 95 year old grandma who has cancer everywhere and is begging for death. It's just unacceptable.
 In the ICU you spend a lot of time keeping corpses alive until their family comes around or their body gives out
In the ICU you spend a lot of time keeping corpses alive until their family comes around or their body gives out
“Oh Jesus ain’t ready for her yet!”
Yes, Jesus is ready for her; we’re just actively delaying it.
 That patient families will do anything to keep the patient alive for their own comfort instead of abiding by the doctors orders. For example: feeding an intubated patient a hamburger because “he’s hungry” when they are already getting tube fed and ordered NOT to interfere with the vent or trach. This has resulted in many patient deaths than you think.
That patient families will do anything to keep the patient alive for their own comfort instead of abiding by the doctors orders. For example: feeding an intubated patient a hamburger because “he’s hungry” when they are already getting tube fed and ordered NOT to interfere with the vent or trach. This has resulted in many patient deaths than you think.
 Nurses can be forced (mandated) to work 16 hour shifts if there’s no other coverage. Many hospitals are understaffed….
Nurses can be forced (mandated) to work 16 hour shifts if there’s no other coverage. Many hospitals are understaffed….
 How much of how I practice medicine is controlled by administration and insurances rather then what makes sense/is best for the patients and how much I hate that.
How much of how I practice medicine is controlled by administration and insurances rather then what makes sense/is best for the patients and how much I hate that.
 Joking about my parents hitting me and getting beat up/in fights to defend myself as a kid always drew looks of horror from my medical school classmates. I would always forget that most of them had physician parents and grew up relatively sheltered haha.
Joking about my parents hitting me and getting beat up/in fights to defend myself as a kid always drew looks of horror from my medical school classmates. I would always forget that most of them had physician parents and grew up relatively sheltered haha.
 Two big ones:
Two big ones:
1) insurance companies dictate everything. Your practice adheres not to evidence but to what will make an insurance company cover appropriate care
2) most people are not practicing evidence based medicine anyway. We develop our habits and stick to them, so even when landmark studies demonstrate we are doing actual harm the average doc doesn’t care and/or never even read the study to begin with. The urgent care mindset of having to give everyone a script overrides good medicine most of the time.
The dark reality of medicine is the insipid political intrigue that goes on that sabotages care for the advancement, wealth and ego of powerful doctors. This means that, as a young physician, you have to take orders from seniors even when they have no idea what they’re doing and even when their actions threaten the welfare of patients. It also means that, to advance to a level of respect where you can actually practice medicine, as opposed to just doing what everyone wants you to do, you have to obsequiously defer to the establishment, to bide your time, even if that establishment consists of dullards who only got their position of authority through patronage of some other powerful authority. I am finally at a level of respect in my profession, critical care, where I can mostly afford to practice as I think best, but it’s taken me years to get there as I looked the other way and let people have their way that shouldn’t be allowed. This reality exists for many professions but in medicine, it threatens lives and isn’t just petty jealousy. There is no meritocracy. You just have to learn to play the game.
1) I was not expecting as much infidelity among doctors tbh.
2) Medical errors or blatant malpractice going uncorrected because of the doctor has the power to ruin the careers of other doctors who point it out
And honestly why are you moving like a cop talking about schools "isn't holding the students accountable for their actions". Not everyone who does d***s like c*ke (op specified in another comment) recreationally is a danger to themselves or patients (and I say this as someone who has never and will never touch it). Only be concerned if direct patient care is being affected.
How often mistakes are made and how easy it can be to make them even with catchalls in place, it’s easy to override. My loved one is admitted right now and they just ordered some thing they don’t normally get. They pushed back and asked why of course that pissed everyone off so they took it. Provider comes in yesterday and apologized profusely saying he didn’t mean to order it for her and was looking at the wrong pt’s ekg while half awake. The most shocking thing to us was that he actually admitted the mistake and apologized.
I worked as a case manager at a for profit long term acute hospital many moons ago. I left because I thought it was very unethical even though I made bank for a social worker. Back then (2013ish), discharge date was determined by DRG payments and totally divorced from what was in the best interest of the patient. I got a printout every morning of when people needed to be discharged by for max profit and at which date we would start losing money. People were often hastily discharged to a lower level of care ready or not when their DRG date came up. Then we got into a length of stay crisis because we were discharging too quick (the rules at the time said an LTACH had to have an average length of stay of 25 days). When this crisis was identified people were kept longer than they needed to be. It was awful. I had a CEO breathing down my throat constantly. I sure hope they have reformed things since then.
The reason you never see dead people being moved is its done very secretly. Hallways are closed down and everyone moved out of the way so the journey from bed to morgue doesn't involve any spectators at all.
Most hospitals also don't have an obvious signpost to the morgue so that people don't get freaked out. But also makes it difficult to find for a viewing.
In a few teaching hospitals some patients are unaware of students practicing invasive examinations on them when they are under.
The hospital covers themselves with vague clauses in the paperwork people sign.
A f****d up practice to be sure.
If you hear your nurse mention they need to run down to the cancer research center don't worry. They're just running for a smoke break.
My sister is a nurse and she’s told me that a lot of nurses and doctors are a******d to d***s (prescription and street d***s).. Some come into work high/drunk.
Lots and lots of mistakes. They had a nursing student give someone a drink before he went into surgery (which he was suppose to have an empty stomach). Also a nursing student accidentally k****d a patient on my sister ward (she wasn’t head nurse). Gave the guy too much pain killers or something like that and k****d him by accident.
When I was a teenager I was placed in the psych ward for a week, and two of the nurses were strangled by two patients.
Counterfeit medical devices make their way into the supply chain. MD companies do everything you can imagine to prevent it, but it happens.
I dunno if this counts as a dark secret but I've had a few ghost experiences in the hospital I used to work at and the staff would try to avoid talking about super natural things happening around the hospital.
An ambulance ride is not a one way ticket to the front of the line. You still get triaged and could be rolled right to the waiting room if you’re non-emergent.
We don't care what your d**k, v****a, b***s etc look like. I have seen literally thousands and can't remember any of them ( except for the one guy whose d**k tip was touching his knee)
Edit: my comment was not saying that people should be comfortable being naked in front of us or that we won't do our best to maintain your level of comfort and keep you as cover as possible.
Hospital lab worker here - Not particularly scandalous, but most people don't realise their lab tests are just very accurate guesses, and have an error range. When we say your 'X' is 10g/L, we might actually mean it's 10g/L ± 10-20%.
I see too many people get extremely worked up about small fluctuations in blood test values that aren't actually in excess of the reference change value, and so technically aren't genuinely different from a previous value.
People abusing nurses and when the nurses report it nothing happens. Nurses deserve safety and the attackers deserve accountability.
I got a fast bleep (ie. drop everything you’re doing and attend this emergency please) one night to a side room on the ward to find no patient in the bed. Was just about to leave the room and go back out to the nurses station, where there had been a bit of a hubbub when I’d dashed past the first time, when something caught my eye.
Looked up to see a face with wide, slightly wild “psych eyes” peering down at me from a gap in the ceiling tiles. She was a lady waiting for a bed in the psych hospital who’d clearly thought the ceiling was the best place to hide from the people trying to poison her.
Honestly can’t think of another occasion that I’ve been quite so terrified.
Worst thing was that I had to walk (well, dash) back out underneath her to get help from the nurses and security to get her down.
Surgeon here. We listen to music in the OR. Most people seem surprised when they hear that.
It’s not uncommon for families to abandon elderly members at the hospital. They will straight up ghost or at least will be polite enough to say they won’t give any assistance to us in placing them in a nursing home, so Adult Protective Services will get involved and make them a ward of the state. This process can take weeks to months, so these abandoned people just live in the hospital and take up the resources that could be used treating sick people.
There are also many families that keep elderly members in unsafe living conditions so they can continue to take their Social Security checks for personal use.
In most older hospitals, the pharmacy is just a couple of feet away from the morgue.
Our's was right off the warehouse loading docks. Only had a capacity for two though.
If you come into the ER drunk there is guaranteed a pool of bets on your blood alcohol level, possibly with odds if there's a pharmacist available to do the math for us.
I help patients to the bathroom nonstop all day. The amount of patients that just leave the bathroom without washing their hands is disgusting. If I didn’t hear the sink or soap dispenser your a*s is getting led right to an alcohol hand station.
The hospital I work at has these big square covers. When I first started, I would see transport staff pushing these things around the halls. I thought they were food trays, or large boxes of hospital equipment. Turns out it’s a structured bed cover, so when they are transporting a deceased patient to the morgue, it doesn’t look like a person under a sheet.
Not hidden, per se, but for the love of all that is holy, if you insist on bringing your kid into the hospital, do NOT let them crawl or play on the floor. The amount of literal blood, urine, p**p, and vomit that has been on it and hastily (not thoroughly) cleaned up is, well, a lot. The hospital, especially the floors, is NOT a clean environment.
Added to that, think of all the rooms nurses, doctors, housekeeping staff, etc. have walked into. Rooms that have COVID or Norovirus or group A Strep. We walked into those rooms and those same shoes walked into other rooms.
Tl;dr hospital floors are disgusting as f**k.
Not really hidden and kinda minor but I’ll say it anyways. I deliver food to patients and it’s not hard to tell when someone is on their way out. Could be simply not being hungry, or could be the inability to eat. Had one patient who hadn’t eaten anything off their tray for 3 days straight. The last time I delivered to them, they smiled and gave me a wink. Next day, they were gone. It’s rough seeing these things happen in real time. I’m a grown a*s man who doesn’t cry often, but it always leaves me feeling extra empty picking up the untouched trays and replacing them with another tray that I know will stay untouched as well.
There is an army of pharmacists in the basement that approve every medication entered by every doctor, frequently catching errors that need a change in therapy (patient on dialysis can’t have x med due to toxicity risk, why is this patient on two nitrate-containing meds?, this patient is 90 and her QTc is already 500 so maybe let’s reconsider the Levaquin, this guy just got that antibiotic in surgery two hours ago so I’ll reschedule it to tomorrow, why is this patient not on blood thinners when they are at high risk for a clotting event, another doctor already ordered potassium repletion for this patient so do you want me to delete your order as a duplicate, you forgot to order a thyroid test before starting amiodarone, this person’s kidney function has stabilized so we can increase their antibiotic dose again, can I change this pantoprazole order to lansoprazole because you can’t crush pantoprazole and the patient has a G-tube, please enter an updated weight for the tiny NICU baby so I can redose all of their weight-based medications, did you really mean to order 1030 units of insulin for this patient or did you want them to get it at 10:30, etc).
When nurses/MDs etc are laughing/joking with each other it is a coping mechanism. We aren't trying to be rude we are compartmentalizing the trauma that we see all day every day. If we don't lighten the load we would cry all day and never come back to work it's literally the only way to watch a baby die and then deal with screaming karen next door with out punching them in the face.
I know one. I used to manage hospital laundry services. Medical waste (body parts etc) gets accidentally thrown in the laundry more often than you'd expect. Also needles and all sorts of other medical devices and personal items. Once we even had a (deceased) fetus come through to the sorting facility.
If you register in the ER and tell the triage nurse that your problem is “personal” we know you’re here because of something genital or a**l related.
Edit: a lot of we healthcare workers have seen a lot. If you’re not truthful at triage, your care might be less prompt when it’s a true medical emergency. It is possible to die of embarrassment.
The lab. The many labs inside a hospital are what you don't know about.
A hospital without a lab is just a bunch of people guessing. A hospital without a lab is a collection of doctors' offices.
Think about that for a moment.
The lab is not where they draw your blood. The lab is where that blood is sent to have various tests. Each color tube does something very specific. Those tubes need to be filled to a certain amount. They need to be drawn in a certain order to keep contamination from causing issues. Sometimes, they even need to be drawn from certain places.
The lab takes your blood, sweat, urine, fluid drainage (from cysts, wounds, around your heart/lungs/liver, brain, etc.), nose swabs, cheek swabs, feces, tumors, removed organs and appendages, growths, and many other unwanted parts and fluids. The lab knows that you eat too much sugar, you lie about that cigarette you enjoy every day, and that you need to stop taking so many over-the-counter pain relievers.
The lab knows when you have chemotherapy. The lab watches your platelet count go down. The lab knows about the deletion of that one gene or the doubling up of another. The lab ran your PCR COVID test and saw you become a statistic. They then asked a blood donor program to hit you up for COVID convalescent plasma, so that you might save a life.
The lab monitored your time on the heart-lung machine. The lab knew when you needed platelets and blood.
The lab saw your lupus diagnosis first. The lab was nearly as upset as you were about it.
The lab was overjoyed when they got the news to pass along to your doctor that the stem cells came in for your bone marrow replacement.
Nurses and doctors see you face to face, but the lab knows you from your insides. The lab is faceless to almost everyone in the hospital (even other staff), which is a shame because the lab is cheering you on in your recovery.
Just because the person seeing you is professional in the room about your weird issue doesn't mean they aren't walking out of there and telling other staff members all about that person that slipped on a bottle and it went in their a*s. No names are used to avoid HIPAA violations but chances are within an hour the entire floor will know about it.
That all the sweet treats and food you bring in for the units to eat usually only go to day shift and night shift gets left out of yummy goodness.
I haven't seen it on here yet, may have missed it but I'll add.
You, as a patient, have every right to refuse any test or treatment or even leave. At any time. For any reason. (Unless a harm to self or others- that's different, at least in the US)
Added bonus you should know: leaving against medical advice DOES NOT mean insurance will not pay for the care you've received. Your insurance will still be billed the same as anyone else who stayed the whole time till discharge.
But if you leave with an IV in your arm we will call the police to find you and bring you back to remove it, because of d**g a***e..
There is s*x and drama, but not in a Grey’s Anatomy way…more of an overgrown high schoolers shoved together in really stressful situations way. And not as much s*x as Grey’s…though maybe I’m just ugly and not in on the scene.
Most don’t judge as much as you you may think. As for myself, a (former) medical professional, I don’t care what d***s you take or how much you drink—I just want the truth so I can provide the best plan of care for you. For example, if you’re an alcoholic or a******d to benzos, I need to know to prepare for possible withdrawals that can become deadly.
In the US, insurance companies are buying up doctor practices, urgent care centers, minute clinics, surgery centers, and pharmacies. This is centralizing all the profit under an organization notorious for screwing over medical providers and patients alike, and there’s a real risk of insurance companies steering their customers toward centers owned by that insurance company without transparency. Hospitals are corrupt enough, but imagine receiving care at one owned by United Health.
Our entire healthcare system is falling apart and insurance companies and big pharma are the only ones winning.
A whole lot of unnecessary suffering that families bring upon their supposed loved ones. Imagine how horrified you’d be if your friend told you they are putting their elder dog Luna on a ventilator because, after her aging achy hips failed her and they did the hip replacement, luna got pneumonia. Of course she can’t eat anymore so they will put a feeding tube in her and feed her. Then they will have people clean her up when she s***s on herself but at least they don’t have to worry that she will pee on herself because after the pneumonia her kidneys failed and now she’s on dialysis. They visit her a couple times each week because they love her.
No. That’s considered inhumane to do to a dog. We do it to millions of elderly humans though.
Imagine being stuck in a windowless white environment with bright florescent lights, beeping machines, pained moaning, and p**p smells for 12 hours. Now do it with less staff than what’s required to manage the volume of people. Now throw in 3 years of burnout from the pandemic.
Now consider how grumpy and frustrated you would be, and consider what would make you stay in the job.
Nurse to patient ratios are now dangerously unsafe. If your nurse has 5+ patients the odds of you dying are like 60% or more. Hospitals can’t hire enough nurses and all of the good ones left due to low wages. Also your nurse may have an inappropriate nursing assignment. This means, the patients are really sick and that nurse shouldn’t have ALL of those patients. This also means some patients who are really sick (think, on life support in the ICU with multiple devices to keep them artificially alive) are not that nurses only patient, when they should be. This also increases the risk of patient harm. Also, a brand new nurse may be given a challenging patient assignment that is extremely inappropriate for them. Due to staffing shortages, this is the only option for the nurse in charge. Many experienced nurses are burnt out and left the bedside, so this has left a lot of inexperienced nurses to be in charge of a unit or taking care of extremely sick patients that they really shouldn’t be.
CEOs, CFOs, or anyone else in the C-suite typically don’t care about patient outcomes, only the hospitals bottom dollar.
The number of assaults on nurses is really high. And nurses are pressured by management to not press charges.
If you don’t have an advanced directive or living will, or don’t know what that is, you should look into one ASAP.
CPR is brutal and many times do not have good outcomes. Many people do not have a good quality of life after these events. I would not want my loved ones to go through CPR.
Don’t distract the nurse or talk about irrelevant things when they’re scanning, hanging, and administering medications. This is a very critical time that the nurse needs to be focused on administering medications. There are certain checks the nurses are required to do. This is the last stop for the nurse to be sure they have the right patient, right d**g, right dose, right route, right frequency, and verifying they’re not giving you a d**g that you’re allergic to.
Just because you see the nurse sitting at the desk doesn’t mean they’re not busy. They are likely documenting care they have provided, checking physician orders and documentation, looking at their schedule, etc.
Nurses very often don’t get 30 minute lunch breaks. Or 15 minute breaks. Or bathroom breaks. Or water breaks. There have been many 12-14 hour shifts I have worked in the ICU where I went to the bathroom 1 time and didn’t drink any water. Oh, and I inhaled my cold lunch in under 5 minutes. If I was afforded that opportunity.
If you see a nurse or hospital staff member running, now is NOT the time to ask them for water, snacks, a blanket, etc. They are likely handling an emergency.
If you are in the ER and someone is actively dying (think, needing CPR, needing immediate life support, actively having a heart attack or stroke, suffering from a life threatening emergency, etc), I don’t care how long you’ve been waiting, they WILL be seen before you even if they have been in that ER for one minute.
The ER is not the place to get an STD test.
Dead bodies are moved to the morgue in special stretchers. You can't see the person at all. It just looks like an empty stretcher.
When the nurses are sitting at the computer " doing nothing " they're documenting. In health care, if it wasn't documented it didn't happen. That means every. Single patient interaction. Needs to be documented , as well as their interaction with the doctors, pharmacy, ect.. they are expected to be a walking transcript of every medical interaction. On top of delivering meds, catching and reporting doctors mistakes, communicating patients preferences to doctors, dietary aides, preforming life saving interventions and arranging pillows just so.....on top of expected to work mandatory overtime. We're talking 16 hr shifts for ...however long. If you see one laughing, or eating, or sitting, it doesn't mean they don't care. They're just not robots. So VOTE for safe patient ratios, and everything that comes with educational encouragement to staff our failing Healthcare system.
ETA: everything is documented, from the regularity of your bowel movements, the respiration(s) ( the amount of time you breathe in a minute) to the color of your p**s, your range of motion, if you're developing a red area, or rash, Anything and everything could be a clue to either a patients deteriorating health, or improvement of health. Multiply that by 3-7 patients depending on what type of unit you're on ( general medical floors versus ICU) and that's why your nurse us at the computer all the time, and if you're surviving, doesn't give a d**n if you're hungry or cold....not enough people for that, at least one of her patients is about to go from bad to worse any minute now.
Most hospitals are dangerously understaffed and cut from very important areas, such as cleaners. So take that information and do with it as you will.
As an x-ray tech, I can’t tell you what’s wrong if you ask me if I see anything on your x-rays because it’s not in our scope of practice, but yeah…we definitely know. And if it’s particularly gruesome, we like to show off how pretty our images came out to other techs lol.
If you’re in a hospital with shared rooms you might have to listen to someone die on the other side of the curtain. Especially if it’s an ICU room. This isn’t as uncommon as you might think it is.
We actually really care about you. You aren’t a number to us and when you have an unexpected outcome, we grieve and have to support each other and have care conferences to process our feelings. Sometimes we even need some time off of work to emotionally recover.
I never knew how much doctors and nurses really cared until I became one.
How often we have to hide how we are made to feel.
Patients blame staff for systemic issues. It’s not your nurses fault the wait time is long, it’s not the individual staff that created the big picture issue. Most of us are trying our best in an unappreciated field and are here trying to help.
A lot of the times we are very friendly and professional with the patient while in the room with them, but as soon as we leave the room we do talks amongst ourselves about what we really thought of you. Very common to leave a room and say to each other “wow that guys an a*****e” or “that wound was freaking nasty” or “that guy is super annoying”.
The updates you get from the OR while your family member is on the table are BS. The case could be going really bad and the OR nurse will still tell you “everything thing is going great”.
As a hospital social worker, a lot of people think "home care" is going to include an insurance covered home health aid. There is no such thing. You have to private hire or get sent to a nursing home for "rehab."
The staff gossip about all the patients' families. It is easy to get labeled aa needy or difficult.
Bringing in food for the staff goes a long way.
Everything falls on the direct care staff. No housekeeping, guess who's swinging a mop. Nutritional services are short, guess who's handing out trays. Security is short and a patient in psychological crisis is strangling their roommate, guess who has less help intervening. If we are short ancillary staff then it's just the RNs to pick up the slack.
Patients family need to understand that we don’t have the time or will to go and get you a cup of coffee or drink at the drop of a hat. There are vending machines and/or a kitchen, go help yourself.
The floors are a hotbed of disease. Always keep your feet covered. Patients walking around barefoot give me the barfs 🤢.
Executives are money/power hogs, operated by a sicophantic clique, and people who are driven by service to human welfare turn over quickly.
Sanitation is suspect and is usually done by people who are in a hurry to clean other rooms. Lots of spots get missed between patients.






















 No fees, cancel anytime
No fees, cancel anytime 






")
")




























